Are Obese Patients with Autism Spectrum Disorder More Likely to Be Selenium Deficient? Research Findings on Pre- and Post-Pubertal Children

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
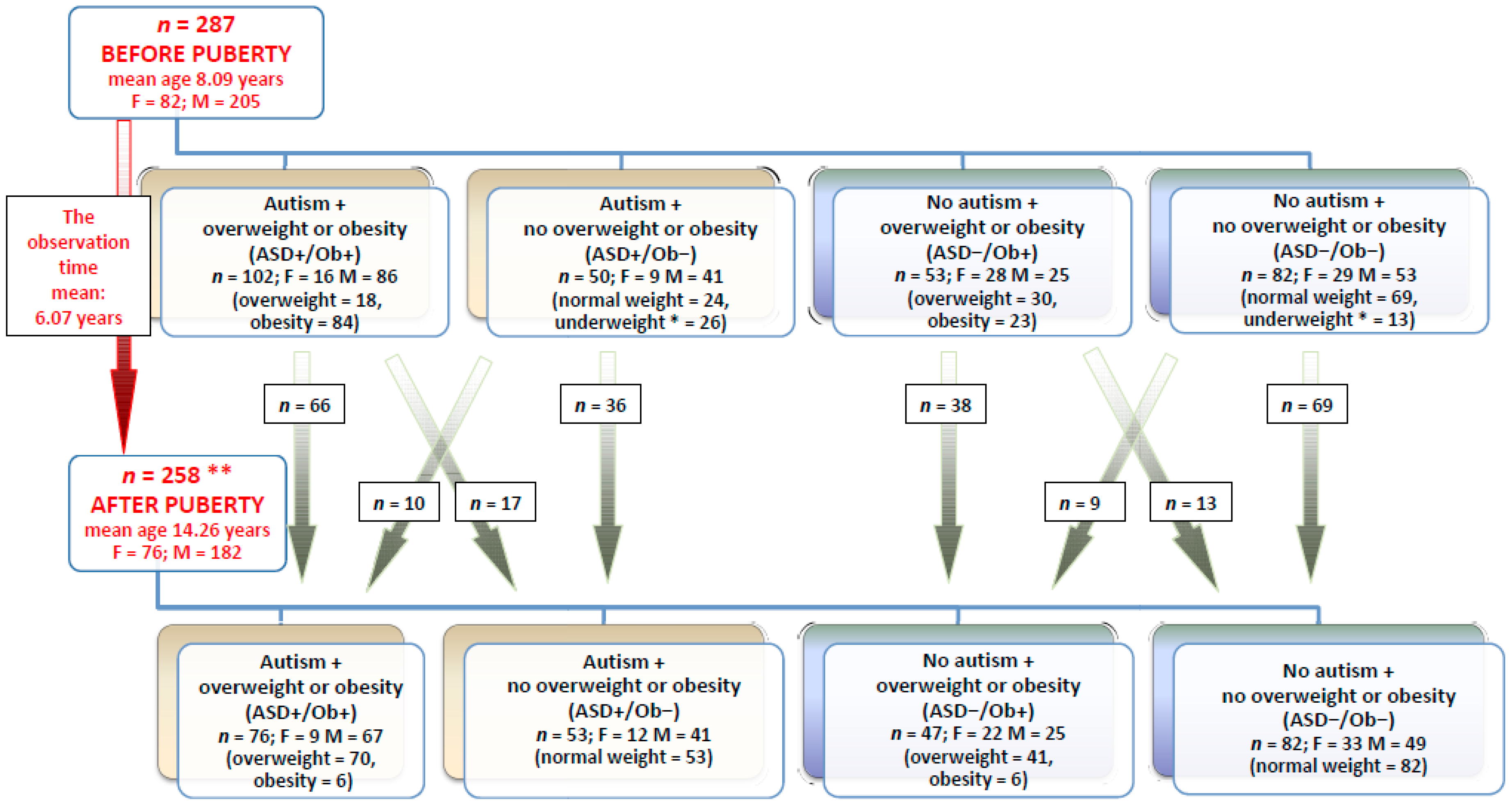
2.1. Study and Control Populations
2.2. Samples and Their Analyses
2.3. Statistical Analyses
3. Results
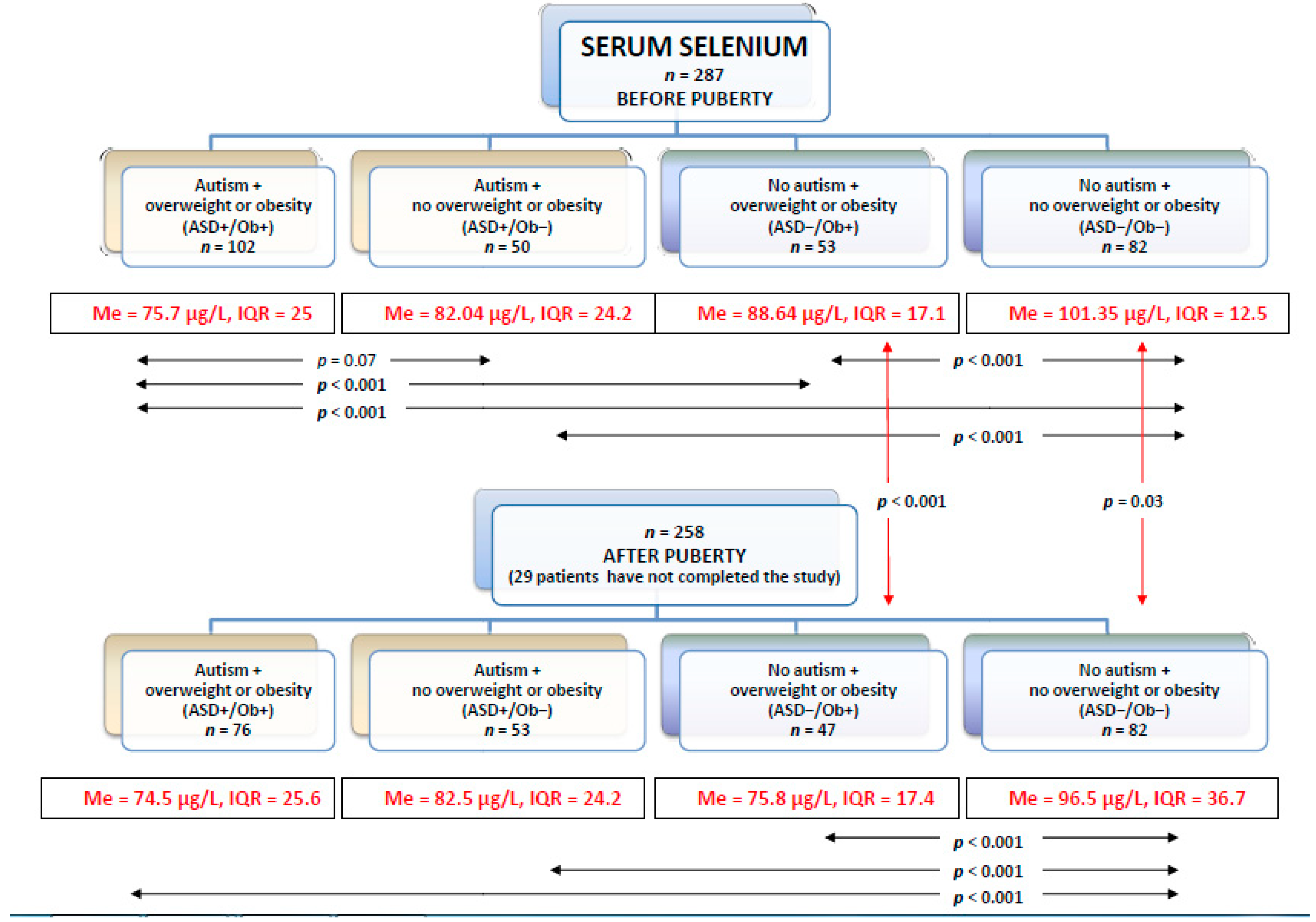
3.1. Selenium in Serum
3.2. Selenium in Urine
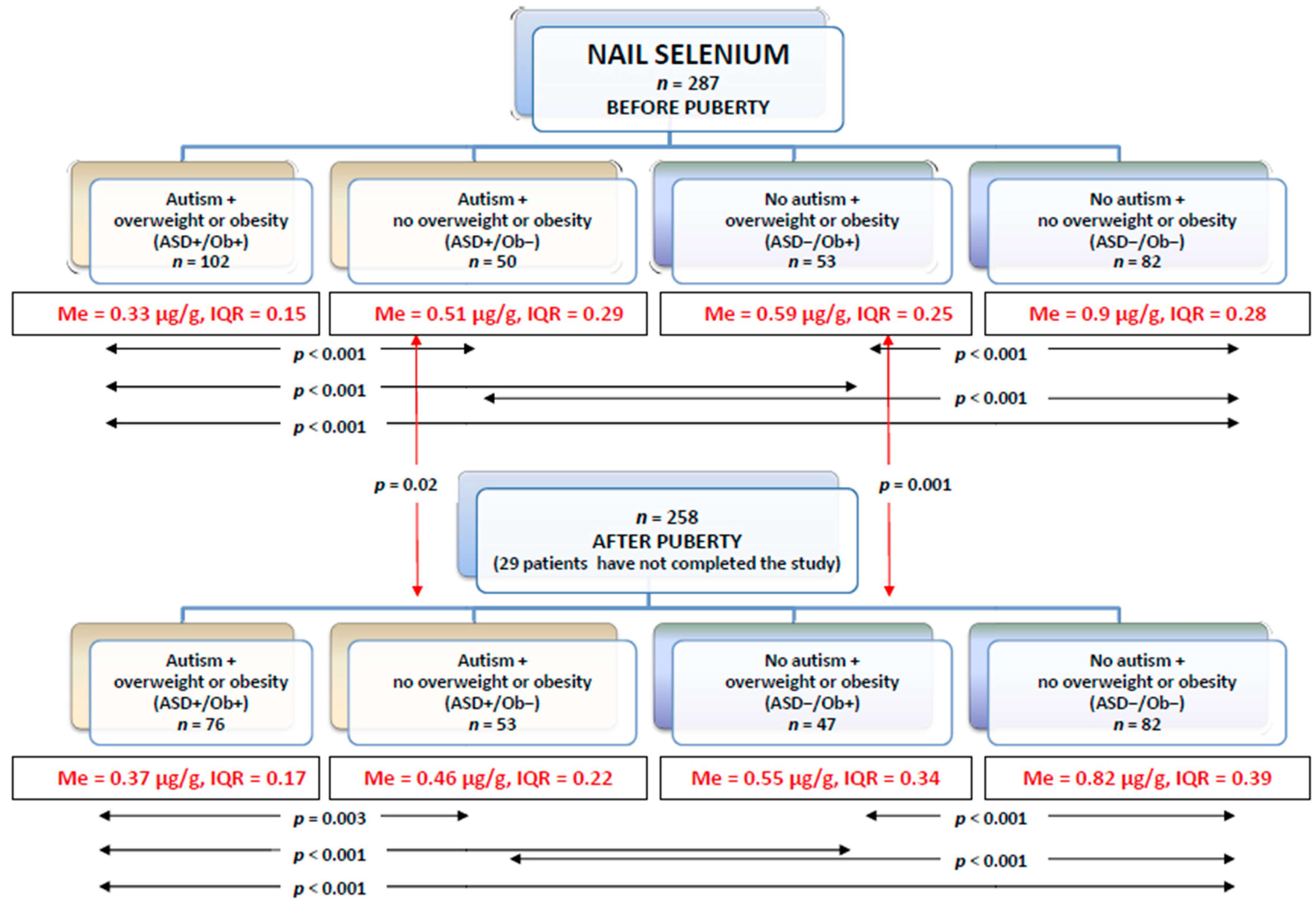
3.3. Selenium in Toenails
3.4. The Spearman’s Correlations between Serum, Urine and Toenail Selenium Concentrations
3.5. Association between Serum, Urine, and Toenail Se Levels and ASD Status, BMI, and Gender
4. Discussion
Advantages and Limitations of the Study
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| ASD | Autism Spectrum Disorder |
| SE | Selenium |
| PDD-NOS | Pervasive Developmental Disorder Not Otherwise Specified |
| AS EDCs | Asperger Syndrome Endocrine disrupting chemicals |
| DSMV | Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition |
| ADI-R | Autism Diagnostic Interview Revised |
| CARS | Autism Rating Scale |
| BMI | Body Mass Index |
| fT3 | Free Triiodothyronine |
| fT4 | Free Thyroxine |
| TSH | Thyroid Stimulating Hormone |
| ICP-MS | Inductively Coupled Plasma Mass Spectrometry |
| IQR | Interquartile Range |
| SD | Standard Deviation |
| SE | Standard Error |
| OR | Odds Ratio |
| CI | Confidence Interval |
References
- Mottron, L.; Bzdok, D. Autism spectrum heterogeneity: Fact or artifact? Mol. Psychiatry 2020, 1–8. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of mental disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Almandil, N.B.; Alkuroud, D.N.; AbdulAzeez, S.; AlSulaiman, A.; Elaissari, A.; Borgio, J.F. Environmental and Genetic Factors in Autism Spectrum Disorders: Special Emphasis on Data from Arabian Studies. Int. J. Environ. Res. Public Health 2019, 16, 658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raymond, L.J.; Deth, R.C.; Ralston, N.V.C. Potential Role of Selenoenzymes and Antioxidant Metabolism in relation to Autism Etiology and Pathology. Autism Res. Treat. 2014, 2014, 1–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Priya, M.D.L.; Geetha, A. Level of Trace Elements (Copper, Zinc, Magnesium and Selenium) and Toxic Elements (Lead and Mercury) in the Hair and Nail of Children with Autism. Biol. Trace Element Res. 2011, 142, 148–158. [Google Scholar] [CrossRef] [PubMed]
- Tschinkel, P.F.S.; Bjørklund, G.; Conón, L.Z.Z.; Chirumbolo, S.; Nascimento, V.A. Plasma concentrations of the trace elements copper, zinc and selenium in Brazilian children with autism spectrum disorder. Biomed. Pharmacother. 2018, 106, 605–609. [Google Scholar] [CrossRef] [PubMed]
- James, S.J.; Cutler, P.; Melnyk, S.; Jernigan, S.; Janak, L.; Gaylor, D.W.; Neubrander, J.A. Metabolicbiomarkers of increased oxidative stress and impaired methylation capacityin children with autism. Am. J. Clin. Nutr. 2004, 80, 1611–1617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jory, J.; McGinnis, W.R. Red-cell trace minerals in children with autism. Am. J. Biochem. Biotechnol. 2008, 4, 101–104. [Google Scholar] [CrossRef]
- Long, M.; Ghisari, M.; Kjeldsen, L.; Wielsøe, M.; Nørgaard-Pedersen, B.; Mortensen, E.L.; Abdallah, M.W.; Bonefeld-Jørgensen, E.C. Autism spectrum disorders, endocrine disrupting compounds, and heavy metals in amniotic fluid: A case-control study. Mol. Autism 2019, 10, 1–19. [Google Scholar] [CrossRef]
- Bjørklund, G.; Skalny, A.V.; Rahman, M.; Dadar, M.; Yassa, H.A.; Aaseth, J.; Chirumbolo, S.; Skalnaya, M.G.; Tinkov, A.A. Toxic metal(loid)-based pollutants and their possible role in autism spectrum disorder. Environ. Res. 2018, 166, 234–250. [Google Scholar]
- Mohamed, F.E.B.; Zaky, E.A.; El-Sayed, A.B.; Elhossieny, R.M.; Zahra, S.S.; Eldin, W.S.; Youssef, W.Y.; Khaled, R.A.; Youssef, A.M. Assessment of hair aluminum, lead, and mercury in a sample of autistic Egyptian children: Environmental risk factors of heavy metals in autism. Behav. Neurol. 2015, 1–9. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Report of the Commission on Ending Childhood Obesity. Implementation Plan: Executive Summary. 2017. Available online: https://apps.who.int/iris/bitstream/handle/10665/259349/WHO-NMH-PND-ECHO-17.1-eng.pdf?sequence=1 (accessed on 18 November 2020).
- James, W.P.T. Obesity: A Global Public Health Challenge. Clin. Chem. 2018, 64, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Hill, A.P.; Zuckerman, K.E.; Fombonne, E. Obesity and autism. Pediatrics 2015, 136, 1051–1061. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamal Nor, N.; Ghozali, A.H.; Ismail, J. Prevalence of Overweight and Obesity Among Children and Adolescents with Autism Spectrum Disorder and Associated Risk Factors. Front. Pediatr. 2019, 7, 38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kummer, A.; Barbosa, I.G.; Rodrigues, D.H.; Rocha, N.P.; Rafael, M.; Pfeilsticker, L.; Silva, A.C.; Teixeira, A.L. Frequency of overweight and obesity in children and adolescents with autism and attention deficit/hyperactivity disorder. Rev. Paul. de Pediatr. 2016, 34, 71–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Curtin, C.; Jojic, M.; Bandini, L.G. Obesity in Children with Autism Spectrum Disorder. Harv. Rev. Psychiatry 2014, 22, 93–103. [Google Scholar] [CrossRef] [Green Version]
- Błażewicz, A.; Klatka, M.; Astel, A.; Korona-Glowniak, I.; Dolliver, W.; Szwerc, W.; Kocjan, R. Serum and urinary selenium levels in obese children: A cross-sectional study. J. Trace Elem. Med. Biol. 2015, 29, 116–122. [Google Scholar]
- Kułaga, Z.; Różdżyńska-Świątkowska, A.; Grajda, A.; Gurzkowska, B.; Wojtyło, M.; Góźdź, M.; Świąder, A.; Litwin, M. Wartości referencyjne wysokości, masy ciała i wskaźnika masy ciała dla oceny wzrastania i stanu odżywienia dzieci i młodzieży w wieku 3–18 lat, 2013, 11. Stand. Med. Pediatr. 2015, 12, 119–135. [Google Scholar]
- Prystupa, A.; Kiciński, P.; Luchowska-Kocot, D.; Błażewicz, A.; Niedziałek, J.; Mizerski, G.; Jojczuk, M.; Ochal, A.; Sak, J.J.; Załuska, W. Association between Serum Selenium Concentrations and Levels of Proinflammatory and Profibrotic Cytokines-Interleukin-6 and Growth Differentiation Factor-15, in Patients with Alcoholic Liver Cirrhosis. Int. J. Environ. Res. Publ. Health 2017, 14, 437. [Google Scholar] [CrossRef]
- Błażewicz, A.; Liao, K.-Y.; Liao, H.-H.; Niziński, P.; Komsta, Ł.; Momčilović, B.; Jabłońska-Czapla, M.; Michalski, R.; Prystupa, A.; Sak, J.J.; et al. Alterations of Hair and Nail Content of Selected Trace Elements in Nonoccupationally Exposed Patients with Chronic Depression from Different Geographical Regions. BioMed Res. Int. 2017, 2017, 1–10. [Google Scholar] [CrossRef]
- Muszyńska, B.; Szacawa, E.; Bederska-Łojewska, D.; Dudek, K.; Pomierny, B.; Włodarczyk, A.; Kała, K.; Lazur, J.; Suchocki, P.; Budziszewska, B.; et al. Preliminary study on Se-enriched Lentinula edodes mycelium as a proposal of new feed additive in selenium deficiency. PLoS ONE 2020, 15, e0233456. [Google Scholar] [CrossRef]
- Tinkov, A.A.; Ajsuvakova, O.P.; Filippini, T.; Zhou, J.-C.; Lei, X.G.; Gatiatulina, E.R.; Michalke, B.; Skalnaya, M.G.; Vinceti, M.; Aschner, M.; et al. Selenium and Selenoproteins in Adipose Tissue Physiology and Obesity. Biomolecules 2020, 10, 658. [Google Scholar] [CrossRef] [PubMed]
- Ortega, R.M.; Rodríguez-Rodríguez, E.; Aparicio, A.; Jiménez-Ortega, A.I.; Palmeros, C.; Perea, J.M.; Navia, B.; López-Sobaler, A.M. Young children with excess of weight show an impaired selenium status. Int. J. Vitam. Nutr. Res. 2012, 82, 121–129. [Google Scholar] [CrossRef] [PubMed]
- Huke, V.; Turk, J.; Saeidi, S.; Kent, A.; Morgan, J.F. Autism Spectrum Disorders in Eating Disorder Populations: A Systematic Review. Eur. Eat. Disord. Rev. 2013, 21, 345–351. [Google Scholar] [CrossRef] [PubMed]
- Figuerola, P.E.; Canals, J.; Fernández-Cao, J.; Val, V.A. Differences in food consumption and nutritional intake between children with autism spectrum disorders and typically developing children: A meta-analysis. Autism 2018, 23, 1079–1095. [Google Scholar] [CrossRef] [PubMed]
- Kalupahana, N.S.; Moustaid-Moussa, N.; Claycombe, K.J. Immunity as a link between obesity and insulin resistance. Mol. Asp. Med. 2012, 33, 26–34. [Google Scholar] [CrossRef]
- Nelson, S.M.; Lei, X.; Prabhu, K.S. Selenium Levels Affect the IL-4–Induced Expression of Alternative Activation Markers in Murine Macrophages. J. Nutr. 2011, 141, 1754–1761. [Google Scholar] [CrossRef] [Green Version]
- Dhanjal, N.I.K.; Sharma, S.; Prabhu, K.S.; Prakash, N.T. Selenium supplementation through Se-rich dietary matrices can upregulate the anti-inflammatory responses in lipopolysaccharide-stimulated murine macrophages. Food Agric. Immunol. 2017, 28, 1374–1392. [Google Scholar] [CrossRef]
- Carlson, B.A.; Yoo, M.-H.; Shrimali, R.K.; Irons, R.; Gladyshev, V.N.; Hatfield, D.L.; Park, J.M. Role of selenium-containing proteins in T-cell and macrophage function. Proc. Nutr. Soc. 2010, 69, 300–310. [Google Scholar] [CrossRef] [Green Version]
- Sivamaruthi, B.S.; Suganthy, N.; Kesika, P.; Chaiyasut, C. The Role of Microbiome, Dietary Supplements, and Probiotics in Autism Spectrum Disorder. Int. J. Environ. Res. Public Health 2020, 17, 2647. [Google Scholar] [CrossRef] [Green Version]
- Fowlie, G.; Cohen, N.; Ming, X. The Perturbance of Microbiome and Gut-Brain Axis in Autism Spectrum Disorders. Int. J. Mol. Sci. 2018, 19, 2251. [Google Scholar] [CrossRef] [Green Version]
- Hrdina, J.; Banning, A.; Kipp, A.P.; Loh, G.; Blaut, M.; Brigelius-Flohé, R. The gastrointestinal microbiota affects the selenium status and selenoprotein expression in mice. J. Nutr. Biochem. 2009, 20, 638–648. [Google Scholar] [CrossRef] [PubMed]
- Sharp, W.G.; Jaquess, D.L.; Lukens, C.T. Multi-method assessment of feeding problems among children with autism spectrum disorders. Res. Autism Spectr. Disord. 2013, 7, 56–65. [Google Scholar] [CrossRef]
- Skalny, A.; Skalnaya, M.; Bjorklund, G.; Gritsenko, V.; Aaseth, J.; Tinkov, A. Selenium and Autism Spectrum Disorder. In Selenium, 1st ed.; Michalke, B., Ed.; Springer: Cham, Switzerland, 2018. [Google Scholar] [CrossRef]
- Spiller, H.A. Rethinking mercury: The role of selenium in the pathophysiology of mercury toxicity. Clin.Toxicol. 2017, 56, 313–326. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Peterson, K.E.; Sánchez, B.N.; Jones, A.D.; Cantoral, A.; Mercado-García, A.; Solano-Gonzalez, M.; Ettinger, A.S.; Téllez-Rojo, M.M. Dietary Intake of Selenium in Relation to Pubertal Development in Mexican Children. Nutrients 2019, 11, 1595. [Google Scholar] [CrossRef] [Green Version]
- Pitts, M.W.; Kremer, P.M.; Hashimoto, A.C.; Torres, D.J.; Byrns, C.N.; Williams, C.S.; Berry, M.J. Competition between the Brain and Testes under Selenium-Compromised Conditions: Insight into Sex Differences in Selenium Metabolism and Risk of Neurodevelopmental Disease. J. Neurosci. 2015, 35, 15326–15338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mayo Clinic Laboratories. Test ID: SES: Selenium, Serum. 1995. Available online: https://www.mayocliniclabs.com/test-catalog/Overview/9765 (accessed on 15 June 2020).
- El-Ansary, A.; Bjørklund, G.; Tinkov, A.A.; Skalny, A.V.; Al Dera, H. Relationship between selenium, lead, and mercury in red blood cells of Saudi autistic children. Metab. Brain Dis. 2017, 32, 1073–1080. [Google Scholar] [CrossRef]
- Tinkov, A.A.; Skalnaya, M.G.; Simashkova, N.V.; Klyushnik, T.P.; Skalnaya, A.A.; Bjørklund, G.; Notova, S.V.; Kiyaeva, E.V.; Skalny, A.V. Association between catatonia and levels of hair and serum trace elements and minerals in autism spectrum disorder. Biomed. Pharmacother. 2019, 109, 174–180. [Google Scholar] [CrossRef]
- Roman, M.; Jitaru, P.; Barbante, C. Selenium biochemistry and its role for human health. Metallomics 2014, 6, 25–54. [Google Scholar] [CrossRef]
- Kieliszek, M. Selenium–Fascinating Microelement, Properties and Sources in Food. Molecules 2019, 24, 1298. [Google Scholar] [CrossRef] [Green Version]
- Arnaud, J.; Weber, J.-P.; Weykamp, C.W.; Parsons, P.J.; Angerer, J.; Mairiaux, E.; Mazarrasa, O.; Valkonen, S.; Menditto, A.; Patriarca, M.; et al. Quality Specifications for the Determination of Copper, Zinc, and Selenium in Human Serum or Plasma: Evaluation of an Approach Based on Biological and Analytical Variation. Clin. Chem. 2008, 54, 1892–1899. [Google Scholar] [CrossRef] [Green Version]
- Filippini, T.; Ferrari, A.; Michalke, B.; Grill, P.; Vescovi, L.; Salvia, C.; Malagoli, C.; Malavolti, M.; Sieri, S.; Krogh, V.; et al. Toenail selenium as an indicator of environmental exposure: A cross-sectional study. Mol. Med. Rep. 2017, 15, 3405–3412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baron-Cohen, S.; Knickmeyer, R.C.; Belmonte, M.K. Sex differences in the brain: Implications for explaining autism. Science 2005, 310, 819–823. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ingudomnukul, E.; Baron-Cohen, S.; Wheelwright, S.; Knickmeyer, R. Elevated rates of testosterone-related disorders in women with autism spectrum conditions. Horm. Behav. 2007, 51, 597–604. [Google Scholar] [CrossRef] [PubMed]
- Pohl, A.; Cassidy, S.; Auyeung, B.; Baron-Cohen, S. Uncovering steroidopathy in women with autism: A latent class analysis. Mol. Autism 2014, 5, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Błażewicz, A.; Szymańska, I.; Astel, A.; Stenzel-Bembenek, A.; Dolliver, W.R.; Makarewicz, A. Assessment of Changes over Time of Lipid Profile, C-Reactive Protein Level and Body Mass Index in Teenagers and Young Adults on Different Diets Belonging to Autism Spectrum Disorder. Nutrients 2020, 12, 2594. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Mean | Median | Min. | Max. | IQR | SD | Mean | Median | Min. | Max. | IQR | SD |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Before Puberty | After Puberty | |||||||||||
| ASD Patients with Overweight or Obesity (ASD+/Ob+) | ||||||||||||
| Age (years) | 7.98 | 8.17 | 6.0 | 10.58 | 2.79 | 1.46 | 14.07 | 14.25 | 12.08 | 16.67 | 2.71 | 1.46 |
| BMI (kg/m2) | 24.8 | 25.51 | 13.21 | 35.16 | 4.96 | 4.97 | 25.96 | 25.7 | 22.66 | 31.14 | 2.32 | 1.83 |
| TSH (µIU/mL) | 2.67 | 2.94 | 0.63 | 4.92 | 1.16 | 0.99 | 3.14 | 3.15 | 0.66 | 5.21 | 2.18 | 1.3 |
| fT4 (pmol/L) | 16.18 | 15.52 | 10.07 | 29.9 | 6.35 | 4.31 | 15.54 | 15.46 | 9.85 | 25.68 | 4.59 | 3.72 |
| fT3 (pmol/L) | 4.83 | 4.55 | 3.55 | 6.95 | 1.03 | 0.84 | 5.03 | 4.99 | 3.78 | 8.12 | 1.26 | 0.89 |
| Se serum (µg/L) | 72.99 | 75.7 | 44.8 | 99.1 | 25.0 | 14.04 | 74.89 | 74.5 | 52.5 | 115.6 | 25.59 | 15.32 |
| Seurine (µg/L) | 41.16 | 40.0 | 25.3 | 69.7 | 11.8 | 9.5 | 45.38 | 45.5 | 22.15 | 70.2 | 20.3 | 12.42 |
| Se toenails (µg/g) | 0.35 | 0.33 | 0,12 | 0.74 | 0.15 | 0.01 | 0.38 | 0.37 | 0.09 | 0.82 | 0.13 | 0.13 |
| ASD Patients Without Overweight or Obesity (ASD+/Ob−) | ||||||||||||
| Age (years) | 7.96 | 8.17 | 6.0 | 10.33 | 2.33 | 1.39 | 14.09 | 14.25 | 12.08 | 17.0 | 2.42 | 1.42 |
| BMI (kg/m2) | 18.31 | 16.15 | 11.96 | 31.99 | 9.18 | 6.01 | 20.47 | 20.66 | 16.76 | 23.11 | 2.15 | 1.6 |
| TSH (µIU/mL) | 2.17 | 2.1 | 0.54 | 4.74 | 2.0 | 1.27 | 1.27 | 0.99 | 0.45 | 3.2 | 0.68 | 0.69 |
| fT4 (pmol/L) | 17.2 | 17.44 | 11.2 | 25.5 | 6.9 | 4.02 | 19.43 | 19.8 | 10.22 | 26.5 | 5.06 | 3.91 |
| fT3 (pmol/L) | 5.32 | 4.96 | 4.15 | 7.11 | 1.71 | 0.97 | 5.78 | 5.6 | 3.99 | 8.11 | 1.72 | 1.04 |
| Se serum (µg/L) | 80.86 | 82.04 | 54.1 | 105 | 24.16 | 14.36 | 80.98 | 82.5 | 52.56 | 112.55 | 24.63 | 15.68 |
| Se urine (µg/L) | 51.68 | 49.8 | 31.5 | 80.55 | 10.75 | 11.68 | 46.53 | 45.5 | 21.56 | 79.5 | 19.0 | 13.79 |
| Se toenails (µg/g) | 0.52 | 0.51 | 0.13 | 0.94 | 0.29 | 0.19 | 0.51 | 0.46 | 0.25 | 0.94 | 0.22 | 0.17 |
| Non-ASD Patients with Overweight or Obesity (ASD−/Ob+) | ||||||||||||
| Age (years) | 8.06 | 7.5 | 6.08 | 10.5 | 2.0 | 1.31 | 14.08 | 13.5 | 12.17 | 16.5 | 2.17 | 1.26 |
| BMI (kg/m2) | 21.62 | 22.7 | 13.77 | 27.77 | 2.4 | 3.79 | 25.89 | 25.46 | 22.19 | 30.67 | 2.18 | 2.07 |
| TSH (µIU/mL) | 2.65 | 2.5 | 0.98 | 4.62 | 1.33 | 0.98 | 2.98 | 2.89 | 1.07 | 4.99 | 1.16 | 0.85 |
| fT4 (pmol/L) | 14.48 | 14.66 | 9.32 | 18.66 | 2.92 | 2.06 | 15.68 | 15.5 | 11.15 | 24.55 | 2.08 | 2.57 |
| fT3 (pmol/L) | 5.07 | 4.99 | 3.95 | 6.78 | 1.01 | 0.75 | 5.17 | 5.12 | 4.26 | 6.71 | 1.04 | 0.68 |
| Se serum (µg/L) | 86.14 | 88.64 | 57.72 | 119.3 | 17.14 | 14.37 | 78.17 | 75.85 | 54.8 | 126.6 | 17.45 | 13.44 |
| Se urine (µg/L) | 40.01 | 38.25 | 23.97 | 59.5 | 12.04 | 8.87 | 45.93 | 45.5 | 32.5 | 65.8 | 10.0 | 6.97 |
| Se toenails (µg/g) | 0.66 | 0.6 | 0.32 | 1.45 | 0.25 | 0.21 | 0.57 | 0.55 | 0.17 | 0.98 | 0.34 | 0.23 |
| Non-ASD Patients Without Overweight or Obesity (ASD−/Ob−) | ||||||||||||
| Age (years) | 8.6 | 8.54 | 6.0 | 10.83 | 1.5 | 1.24 | 14.6 | 14.67 | 12.08 | 16.83 | 1.5 | 1.24 |
| BMI (kg/m2) | 17.05 | 16.52 | 11.9 | 23.99 | 3.12 | 2.54 | 20.73 | 20.66 | 18.7 | 23.46 | 1.83 | 1.22 |
| TSH (µIU/mL) | 1.39 | 1.1 | 0.5 | 3.98 | 1.25 | 0.71 | 1.61 | 1.47 | 0.17 | 3.87 | 1.41 | 0.89 |
| fT4 (pmol/L) | 16.6 | 16.47 | 11.6 | 24.45 | 4.63 | 2.92 | 17.1 | 16.54 | 11.25 | 24.25 | 5.1 | 3.11 |
| fT3 (pmol/L) | 5.43 | 5.28 | 4.01 | 6.74 | 1.19 | 0.73 | 5.35 | 5.23 | 4.2 | 6.7 | 1.0 | 0.66 |
| Se serum (µg/L) | 104.93 | 101.35 | 66.3 | 149.5 | 12.5 | 15.27 | 98.8 | 96.52 | 62.48 | 145.2 | 36.68 | 20.66 |
| Se urine (µg/L) | 52.36 | 50.85 | 38.1 | 69.5 | 9.5 | 7.2 | 50.54 | 50.17 | 32.5 | 89.6 | 10.4 | 8.67 |
| Se toenails (µg/g) | 0.97 | 0.9 | 0.24 | 1.96 | 0.28 | 0.34 | 0.86 | 0.82 | 0.4 | 1.92 | 0.39 | 0.33 |
| Variablesi | Before Puberty | After Puberty | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Total | ASD+/Ob+ | ASD+/Ob− | ASD−/Ob+ | ASD−/Ob− | Total | ASD+/Ob+ | ASD+/Ob− | ASD−/Ob+ | ASD−/Ob− | |
| n = 287 | n = 102 | n = 50 | n = 53 | n = 82 | n = 258 | n = 76 | n = 53 | n = 47 | n = 82 | |
| Age (years) & Se serum (µg/L) | R = 0.15 p = 0.012 | R= −0.38 p < 0.001 | R = 0.34 p = 0.016 | R = 0.26 p = 0.06 | R = 0.08 p = 0.46 | R= −0.02 p = 0.75 | R= −0.25 p = 0.03 | R = 0.18 p = 0.2 | R= −0.15 p = 0.32 | R= −0.17 p = 0.12 |
| Age (years) & Se urine (µg/L) | R = 0.13 p = 0.03 | R= −0.18 p = 0.07 | R = 0.51 p < 0.001 | R = 0.31 p = 0.02 | R = 0.006 p = 0.96 | R = 0.02 p = 0.73 | R= −0.24 p = 0.03 | R = −0.04 p = 0.78 | R = 0.13 p = 0.39 | R = 0.29 p = 0.008 |
| Age (years) & Se toenails (µg/g) | R = 0.17 p = 0.004 | R = 0.02 p = 0.84 | R= −0.15 p = 0.3 | R = 0.37 p = 0.006 | R= −0.09 p = 0.44 | R = 0.04 p = 0.5 | R = 0.09 p = 0.42 | R = −0.19 p = 0.18 | R = 0.01 p = 0.97 | R= −0.22 p = 0.042 |
| BMI (kg/m2) & Se serum (µg/L) | R = −0.47 p < 0.001 | R = −0.32 p = 0.001 | R = 0.31 p = 0.03 | R = −0.6 p < 0.001 | R = 0.04 p = 0.68 | R = −0.46 p < 0.001 | R = −0.49 p < 0.001 | R = 0.16 p = 0.26 | R = −0.55 p < 0.001 | R = −0.29 p = 0.008 |
| BMI (kg/m2) & Se urine (µg/L) | R = −0.52 p < 0.001 | R = −0.26 p = 0.007 | R = 0.25 p = 0.08 | R = −0.39 p = 0.004 | R = −0.06 p = 0.61 | R = −0.18 p = 0.003 | R = −0.24 p = 0.04 | R = 0.09 p = 0.5 | R = −0.12 p = 0.43 | R= −0.07 p = 0.51 |
| BMI (kg/m2) & Se toenails (µg/g) | R = −0.51 p < 0.001 | R = −0.04 p = 0.7 | R = −0.19 p = 0.19 | R = −0.29 p = 0.03 | R = −0.05 p = 0.67 | R = −0.52 p < 0.001 | R = −0.35 p = 0.002 | R = −0.11 p = 0.42 | R = −0.54 p < 0.001 | R = −0.25 p = 0.02 |
| TSH (µIU/mL) & Se serum (µg/L) | R = −0.42 p < 0.001 | R = 0.08 p = 0.43 | R = −0.17 p = 0.24 | R = −0.59 p < 0.001 | R = −0.02 p = 0.82 | R= −0.22 p < 0.001 | R= −0.28 p = 0.01 | R = 0.37 p = 0.006 | R= −0.31 p = 0.03 | R = 0.19 p = 0.08 |
| TSH (µIU/mL) &Se urine (µg/L) | R = −0.38 p < 0.001 | R = 0.0001 p = 0.999 | R = −0.27 p = 0.06 | R = −0.42 p = 0.002 | R = −0.07 p = 0.51 | R = −0.15 p = 0.01 | R = −0.04 p = 0.74 | R = 0.23 p = 0.09 | R = −0.14 p = 0.33 | R = 0.2 p = 0.07 |
| TSH (µIU/mL) & Se toenails (µg/g) | R = −0.46 p < 0.001 | R = −0.17 p = 0.094 | R = −0.2 p = 0.17 | R = −0.46 p < 0.001 | R = −0.08 p = 0.48 | R = −0.32 p < 0.001 | R = −0.33 p = 0.003 | R = −0.02 p = 0.9 | R = −0.33 p = 0.02 | R = 0.14 p = 0.22 |
| fT4 (pmol/L) & Se serum (µg/L) | R = 0.04 p = 0.49 | R = −0.02 p = 0.81 | R= −0.1 p = 0.49 | R = 0.39 p = 0.004 | R = −0.04 p = 0.73 | R = 0.13 p = 0.04 | R = 0.28 p = 0.01 | R = −0.29 p = 0.034 | R = 0.14 p = 0.36 | R = 0.06 p = 0.57 |
| fT4 (pmol/L) & Se urine (µg/L) | R = 0.03 p = 0.63 | R = −0.14 p = 0.16 | R = −0.09 p = 0.55 | R = 0.07 p = 0.63 | R = 0.04 p = 0.75 | R = 0.08 p = 0.19 | R = 0.21 p = 0.07 | R = −0.07 p = 0.61 | R = −0.16 p = 0.28 | R = 0.02 p = 0.88 |
| fT4 (pmol/L) & Se toenails (µg/g) | R = 0.07 p = 0.23 | R = −0.01 p = 0.9 | R = 0.13 p = 0.38 | R = 0.42 p = 0.002 | R = 0.02 p = 0.84 | R = 0.16 p = 0.009 | R = 0.23 p = 0.04 | R = 0.03 p = 0.85 | R = 0.14 p = 0.35 | R = −0.06 p = 0.57 |
| fT3 (pmol/L) & Se serum (µg/L) | R = 0.23 p < 0.001 | R = 0.06 p = 0.56 | R = −0.1 p = 0.5 | R = 0.16 p = 0.26 | R = −0.23 p = 0.04 | R = 0.15 p = 0.02 | R = 0.26 p = 0.02 | R = −0.17 p = 0.23 | R = 0.22 p = 0.14 | R = 0.15 p = 0.17 |
| fT3 (pmol/L) & Se urine (µg/L) | R = 0.26 p < 0.001 | R = −0.13 p = 0.17 | R = 0.23 p = 0.11 | R = 0.16 p = 0.24 | R = 0.05 p = 0.66 | R = 0.15 p = 0.01 | R = 0.22 p = 0.06 | R = 0.1 p = 0.47 | R = 0.12 p = 0.42 | R = 0.07 p = 0.54 |
| fT3 (pmol/L) & Se toenails (µg/g) | R = 0.32 p < 0.001 | R = 0.008 p = 0.94 | R = −0.09 p = 0.52 | R = 0.27 p = 0.049 | R = 0.28 p = 0.01 | R = 0.21 p < 0.001 | R = 0.31 p = 0.007 | R = −0.11 p = 0.43 | R = 0.17 p = 0.25 | R = 0.19 p = 0.09 |
| Se serum (µg/L) &Se urine (µg/L) | R = 0.5 p < 0.001 | R = 0.34 p < 0.001 | R = 0.58 p < 0.001 | R = 0.35 p = 0.009 | R = 0.03 p = 0.76 | R = 0.43 p < 0.001 | R = 0.50 p < 0.001 | R = 0.31 p = 0.02 | R = 0.3 p = 0.039 | R = 0.28 p = 0.01 |
| Se serum (µg/L) & Se toenails (µg/g) | R = 0.56 p < 0.001 | R = 0.12 p = 0.24 | R = −0.13 p = 0.36 | R = 0.27 p = 0.049 | R = −0.011 p = 0.92 | R = 0.49 p < 0.001 | R = 0.26 p = 0.02 | R = −0.19 p = 0.17 | R = 0.59 p < 0.001 | R = 0.59 p < 0.001 |
| Se urine (µg/L) & Se toenails (µg/g) | R = 0.28 p < 0.001 | R = −0.17 p = 0.09 | R = −0.07 p = 0.64 | R = 0.05 p = 0.71 | R = 0.08 p = 0.46 | R = 0.25 p < 0.001 | R = 0.21 p = 0.07 | R = 0.13 p = 0.36 | R = 0.24 p = 0.10 | R = 0.19 p = 0.08 |
| Total n = 258 | ASD+/Ob+ n = 83 | ASD+/Ob− n = 46 | ASD−/Ob+ n = 51 | ASD−/Ob− n = 78 | |
|---|---|---|---|---|---|
| Se serum before puberty (µg/L) & Se serum after puberty (µg/L) | R= 0.49 p< 0.001 | R= 0.42 p< 0.001 | R= 0.5 p< 0.001 | R = 0.25 p = 0.08 | R = 0.16 p = 0.16 |
| Se urine before puberty (µg/L) & Se urine after puberty (µg/L) | R= 0.47 p< 0.001 | R= 0.43 p< 0.001 | R= 0.55 p< 0.001 | R= 0.31 p= 0.02 | R= 0.41 p< 0.001 |
| Selenium toenails before puberty (µg/g) & Se toenails after puberty (µg/g) | R= 0.71 p< 0.001 | R = 0.15 p = 0.18 | R= 0.99 p< 0.001 | R= 0.3 p= 0.03 | R= 0.3 p= 0.007 |
| Multivariate Linear Regression | |||||
|---|---|---|---|---|---|
| n = 258 | BETA | SE a of BETA | B | SE a of B | p-Value |
| Selenium Serum (µg/L) | |||||
| ASD b (ASD 1, no ASD 0) | −0.15 | 0.05 | −6.04 | 1.89 | 0.002 |
| Gender (male 1; female 0) | −0.47 | 0.05 | −20.33 | 2.04 | <0.001 |
| BMI c (kg/m2) | −0.39 | 0.05 | −2.44 | 0.29 | <0.001 |
| Selenium Urine (µg/L) | |||||
| ASD b (ASD 1, no ASD 0) | −0.02 | 0.06 | −0.37 | 1.36 | 0.79 |
| Gender (male 1; female 0) | −0.34 | 0.06 | −8.25 | 1.46 | <0.001 |
| BMI c (kg/m2) | −0.13 | 0.06 | −0.44 | 0.21 | 0.03 |
| Selenium Toenails (µg/g) | |||||
| ASD b (ASD 1, no ASD 0) | −0.39 | 0.05 | −0.24 | 0.03 | <0.001 |
| Gender (male 1; female 0) | −0.26 | 0.05 | −0.18 | 0.03 | <0.001 |
| BMI c (kg/m2) | −0.39 | 0.05 | −0.04 | 0.004 | <0.001 |
| Logistic Regression | |||||
| n = 258 | d OR | e 95% CI | p-Value | ||
| b ASD (modeled probability that: b ASD 1, neurotypical 0 = 1) | |||||
| Selenium serum (µg/L) | 0.97 | 0.95 to 0.99 | 0.003 | ||
| Selenium urine (µg/L) | 1.002 | 0.97 to 1.04 | 0. 87 | ||
| Selenium toenails (µg/g) | 0.0009 | 0.0001 to 0.006 | <0.001 | ||
| Obesity/Overweight (modeled probability that: obesity/overweight 1, normal weight 0 = 1) | |||||
| Selenium serum (µg/L) | 0.95 | 0.93 to 0.97 | <0.001 | ||
| Selenium urine (µg/L) | 1.002 | 0.98 to 1.03 | 0.86 | ||
| Selenium toenails (µg/g) | 0.01 | 0.003 to 0.046 | <0.001 | ||
| Gender (modeled probability that: male 1, female 0 = 1) | |||||
| Selenium serum (µg/L) | 0.93 | 0.91 to 0.95 | <0.001 | ||
| Selenium urine (µg/L) | 0.95 | 0.92 to 0.98 | 0.002 | ||
| Selenium toenails (µg/g) | 0.045 | 0.015 to 0.13 | <0.001 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Błażewicz, A.; Szymańska, I.; Dolliver, W.; Suchocki, P.; Turło, J.; Makarewicz, A.; Skórzyńska-Dziduszko, K. Are Obese Patients with Autism Spectrum Disorder More Likely to Be Selenium Deficient? Research Findings on Pre- and Post-Pubertal Children. Nutrients 2020, 12, 3581. https://doi.org/10.3390/nu12113581
Błażewicz A, Szymańska I, Dolliver W, Suchocki P, Turło J, Makarewicz A, Skórzyńska-Dziduszko K. Are Obese Patients with Autism Spectrum Disorder More Likely to Be Selenium Deficient? Research Findings on Pre- and Post-Pubertal Children. Nutrients. 2020; 12(11):3581. https://doi.org/10.3390/nu12113581
Chicago/Turabian StyleBłażewicz, Anna, Iwona Szymańska, Wojciech Dolliver, Piotr Suchocki, Jadwiga Turło, Agata Makarewicz, and Katarzyna Skórzyńska-Dziduszko. 2020. "Are Obese Patients with Autism Spectrum Disorder More Likely to Be Selenium Deficient? Research Findings on Pre- and Post-Pubertal Children" Nutrients 12, no. 11: 3581. https://doi.org/10.3390/nu12113581