
Abstract
Fluoride exposure is associated with later pubertal development and decreased testosterone production in adolescent and adult males. However, its effects on female reproductive health and pubertal development are unclear. Therefore, we examined associations of fluoride exposure with reproductive health outcomes among adolescent girls and women in the United States. Participants were from The National Health and Nutrition Examination Surveys (2013 to 2016), aged 16–19 and identified as female. There were 524 and 460 participants with measures of plasma fluoride and household tap water fluoride respectively, who had at least one reproductive health outcome examined, and complete covariate data. We applied covariate adjusted survey-weighted linear or logistic regression to examine associations of fluoride exposure with age of menarche, menstrual cycle regularity, or serum sex steroid hormone levels. Median interquartile range (IQR) water and plasma fluoride concentrations were 0.48 (0.53) mg/L and 0.34 (0.30) µmol/L respectively. An IQR increase in water fluoride was associated with a 3.3 month earlier first menstrual period (B = − 0.28, 95%CI − 0.54, − 0.02, p = 0.05). Additionally, we observed a significant interaction between plasma fluoride and race/ethnicity in association with age of menarche (p = 0.01). Among Non-Hispanic Black adolescents, each IQR increase in plasma fluoride was associated with a 5-month earlier age of menarche (B = − 0.42, 95%CI − 0.61, − 0.23, p < 0.001). Potential impacts of chronic low-level fluoride exposure on reproductive health outcomes are an important area of study. Current study findings, as well as potential health disparities due to disproportionate fluoride exposure should be examined in prospective studies.
Similar content being viewed by others

Introduction
Fluoride exposure is widespread in the United States (US) as well as other developed and developing countries. In the US, approximately 73% of the population on public water distribution systems receives fluoridated water for tooth decay prevention (CDC 2018a, b, c). Fluoridated water accounts for approximately 40% and 60% of fluoride intake among US children and adults respectively (US Environmental Protection Agency (USEPA) 2010). Although the dental benefits of fluoride are well-established, in 2006, a National Research Council report concluded that fluoride is an endocrine disruptor that can alter normal endocrine function or response (National Research Council 2006).
There is substantial evidence that endocrine disrupting chemicals (EDCs) can adversely affect reproductive health and may alter timing of pubertal onset (Sifakis et al. 2017; Greenspan and Lee 2018; Lee et al. 2019; Lucaccioni et al. 2020). Moreover, animal studies show that fluoride exposure can decrease testosterone production and adversely affect testicular and ovarian development (Kinawy and Al-Eidan 2018; Orta Yilmaz et al. 2018; Chaithra et al. 2020; Li et al. 2020). Studies conducted in China have also found associations of fluoride exposure with decreased testosterone production in men (Susheela and Jethanandani 1996; Duan et al. 2016), lower estrogen levels in women (Chen et al. 2015) and male infertility in regions with endemic fluorosis (Liu 1988).
Research suggests that fluoride exposure may influence reproductive health among youth. A recent NHANES study found that higher plasma fluoride levels were associated with lower testosterone, estradiol and serum hormone binding globulin (SHBG) levels in adolescent boys as well as lower SHBG in girls (Bai et al. 2020a, b). Another recent study conducted in Mexico City found that higher urine fluoride levels were associated with later pubertal development among boys but were not significantly associated with pubertal development or age of menarche in girls (Liu et al. 2019a, b). Two prior ecological studies conducted in the US and Hungary reported putative evidence of earlier menarche among girls in relation to water fluoride exposure (Schlesinger et al. 1956; Farkas et al. 1983), although these ecological studies could not adjust for important confounders, and trends detected were not significant. Therefore, given the scarce data on fluoride exposure and women’s reproductive health or pubertal development, our study explored associations of plasma and water fluoride concentrations with age of menarche, menstrual cycle regulatory and serum sex steroid hormone levels among adolescent girls and women in the United States.
Methods
Participants
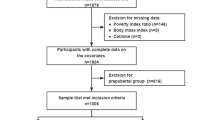
We included participants from the National Health and Nutrition Examination Survey (NHANES) cycles between 2013 and 2016—the years for which publicly available fluoride biomonitoring data were available. Plasma fluoride concentrations were measured among 4470 participants aged 6–19 years and tap water fluoride concentrations were measured among 8087 participants aged 0–19 years. We included adolescent girls/women aged 16–19 years in our analysis as all participants within this age range had experienced menarche. We included participants who had either plasma or water fluoride measurements, complete covariate data, as well as data for at least one reproductive health outcome. Missing data were < 15% for covariates among participants who had at least one outcome measure. Additionally, we excluded participants who were taking estradiol-based medications that could affect sex hormone levels (n = 46 and n = 41 for plasma and water fluoride samples respectively) only for analyses that included serum sex steroid hormone levels or menstrual regularity as outcomes. There were 524 participants with plasma fluoride levels who met inclusion criteria and 553 participants with water fluoride levels who met inclusion criteria. Additionally, for analyses with water fluoride, we excluded an additional 93 participants who reported that they did not drink tap water, which resulted in a sample size of 460. Participant selection is depicted in Figure S1. Supplemental Table S1 compares demographic characteristics of the current study sample meeting inclusion criteria (n = 567) with all adolescent girls and women ages 16–19 in NHANES 2013–2016. We applied sampling weights to account for the complex NHANES survey design as recommended by the National Center for Health Statistics (NCHS) (Centers for Disease Control and Prevention 2013). The weighted samples for plasma and water fluoride analyses represented 6,555,145 and 6,854,071 adolescents in the U.S. respectively. This study was exempt from review by the Icahn School of Medicine at Mount Sinai’s (ISMMS) Institutional Review Board (#1702145).
Fluoride Measures
Fluoride concentrations were measured in blood plasma and household tap water samples. Tap water and blood collection times were not standardized. Plasma fluoride was measured via an ion-specific electrode and hexamethyldisiloxane (HMDS) method, and household water samples were measured via an ion-specific electrode (NHANES 2017a, b). Both plasma and water fluoride concentrations were measured at the College of Dental Medicine, Georgia Regents University, Augusta, GA. Each sample was measured in duplicate and the average of the two values was reported (NHANES 2017a, b). The lower limit of detection (LLOD) for plasma fluoride was 0.25 nmol, while the LLOD for water fluoride was 0.10 mg/L. Approximately 89% and 100% (all) of participants, had water and plasma fluoride values above the LLOD, respectively (NHANES 2016a, b, 2017a, b).
Serum Sex Steroid Hormones
Estradiol and Testosterone
Estradiol and testosterone contribute to the development of secondary sex characteristics in females and males respectively. Additionally, elevated testosterone levels in females can reflect adrenal hyperplasia, polycystic ovarian syndrome (PCOS), ovarian or adrenal tumors, or ovarian insufficiency. Testosterone and estradiol were measured via isotope dilution liquid chromatography tandem mass spectrometry (ID-LC–MS/MS), a method based on the National Institute for Standards and Technology’s (NIST) reference. The standard reference range for testosterone among adult women is 15–70 ng/dL, while the standard reference range for estrogen fluctuates throughout the menstrual cycle (CDC 2018a). For example, normal levels range from 20–150 pg/mL during the early follicular phase and peak at 150–750 pg/mL during the mid-cycle peak (CDC 2018a).
Serum Hormone Binding Globulin (SHBG)
Serum hormone binding globulin is the blood transport protein for androgens and estrogens. Decreased serum SHBG is associated with hypothyroidism, PCOS, obesity, hirsutism, elevated androgen levels, alopecia, acromegaly, as well as SHBG gene polymorphisms. Elevated serum SHBG is linked with hyperthyroidism, cirrhosis of the liver, and polymorphisms in the SHBG gene (Bhasin et al. 2018; NHANES 2018). SHBG levels were measured via a reaction with immuno-antibodies as well as chemo-luminescence measurements of the reaction products that occur after two incubation periods and subjection to a magnetic field. Through this process, the microparticles were captured on an electrode, where a chemiluminescent reaction occurs, and measured by a photomultiplier tube (CDC 2018b).
Reproductive Health
Participants were asked how old they were when they experienced menarche (i.e., How old {were you/was SP} when {you/SP} had {your/her} first menstrual period?) as well as whether they had regular menstrual periods in the last 12 months (i.e., operationalized as {Have you/Has SP} had at least one menstrual period in the past 12 months?).
Covariates
Covariates were selected a priori based on prior empirical evidence associated with fluoride exposure and women’s reproductive health outcomes. They included age, Body Mass Index (BMI), race/ethnicity and the ratio of family income to poverty (Chumlea et al. 2003; Kaplowitz 2008; Braithwaite et al. 2009; Martinez-Mier and Soto-Rojas 2010; Villa et al. 2010; Jain 2017; Liu et al. 2019a, b). We grouped the race/ethnicity variable into the following categories: Hispanic, Non-Hispanic White, Non-Hispanic Black, and Other to account for small sample sizes of certain racial/ethnic groups. We utilized raw BMI values and the ratio of family income to poverty was calculated by dividing annual family income by the poverty guidelines for the survey year. Poverty guidelines established by the Department of Health and Human Services were utilized to calculate this ratio. These guidelines vary according to family size and geographic location (U.S. Department of Health & Human Services).
Statistical Analysis
All analyses applied mobile exam center (MEC) survey weights to account for the NHANES survey design and to permit generalization to the United States population (National Center for Health Statistics 2013). MEC weights were reweighted to our sample using an adjustment factor prior to analyses according to NCHS guidance (Malin et al. 2019). Descriptive statistics and regression analyses were performed using SAS (V.9.4) software.
For regression analyses we included laboratory generated values for water fluoride that were below the LLOD; however, we imputed water fluoride values below the LLOD as LLOD/ √2 in our calculation of descriptive statistics, according to the CDC’s published data analysis methods (CDC 2017). We explored potentially influential values using a Cook’s Distance estimate and did not identify any. For regression models testing associations of plasma or water fluoride with age of menarche or menstrual cycle regularity, assumptions pertaining to normality, homogeneity of variance and linearity were satisfied. However, regression assumptions were not satisfied for models examining associations of water or plasma fluoride with serum sex steroid hormones. Therefore, we applied a log2 transformation to skewed serum sex steroid hormone variables to satisfy assumptions. We applied covariate adjusted survey-weighted linear or logistic regression to explore associations of fluoride exposure with age of menarche, menstrual cycle regularity, or serum sex steroid hormone levels. We calculated the interquartile range (IQR) for both plasma and water fluoride and presented results of regression analyses in terms of an IQR increase in plasma or water fluoride level. We also included a fluoride*race/ethnicity interaction term in our models to test for effect modification by race/ethnicity using Non-Hispanic White as the reference. This interaction term was only retained in models for which it was significant. When the interaction term was significant, we examined slopes within the ethnic/racial group strata. A two-tailed alpha of 0.05 was the criterion for statistical significance for regression analyses.
Results
Descriptive statistics for demographic characteristics are presented in Table 1. The average age of participants was approximately 17 years and the majority identified as Non-Hispanic White. Table 2 presents descriptive statistics for fluoride exposure variables for the overall plasma and water fluoride samples and according to race/ethnicity. The median household water fluoride concentration among participants who drank tap water was 0.48 mg/L which is below the Public Health Service recommended drinking water level of 0.70 mg/L (United States Department of Health and Human Services—Federal Panel on Community Water Fluoridation 2015) however, the 75th percentile of 0.71 mg/L was slightly above this level. Although not statistically significant, higher median household tap water and plasma fluoride concentrations were observed among Non-Hispanic Black participants compared to other racial and ethnic demographic groups (Table 2; Supplemental Figure S2).
Associations Between Fluoride Exposure and Sex Steroid Hormone Levels
In linear regression models adjusted for covariates, neither plasma nor water fluoride levels were associated with any of the serum sex steroid hormone outcomes examined (see Table 3).
Associations Between Fluoride Exposure and Menstrual Cycle Start or Regularity
Regression results for associations of water fluoride matrices with reproductive health outcomes are presented in Table 4. In linear regression models adjusted for covariates, higher water fluoride concentrations were associated with earlier age of menarche (B: − 0.28, 95%CI − 0.54, − 0.02, p = 0.05) such that each 0.53 mg/L increase in household tap water fluoride concentration was associated with a 3.3-month earlier menarche (see Fig. 1). In linear regression models adjusted for covariates, we did not observe significant associations of plasma fluoride with age of menarche in the overall sample. However, we observed a significant interaction between plasma fluoride and race/ethnicity in association with age of menarche (p = 0.01), such that higher plasma fluoride concentrations were associated with earlier age of menarche among Non-Hispanic Black adolescents. Specifically, for Non-Hispanic Black adolescent girls and women, each IQR (i.e., 0.30 µmol/L) increase in plasma fluoride was associated with a 5-month earlier age of menarche (B: − 0.42, 95%CI − 0.62, − 0.22, p < 0.001) (Fig. 2). We did not observe significant associations between fluoride exposure matrices and menstrual cycle regularity.

Bubble plot of associations of plasma fluoride and water fluoride with age of menarche. Size of bubbles reflects the magnitude of sampling weights. N = 446 for the water fluoride sample and N = 504 for the plasma fluoride sample. Units are umol/L for plasma fluoride and mg/L for water fluoride. Descriptive caption The figure depicts two regression lines—one in red representing plasma fluoride concentration and one in blue representing water fluoride concentration. There are red and blue circles corresponding to data points for plasma and water fluoride respectively and the size of these circles reflects the magnitude of sampling weights. Fluoride concentration is depicted along the horizontal axis while age of menarche is depicted along the vertical axis. As water fluoride level increases, age of menarche decreases (shown by a slightly descending blue line); however, as plasma fluoride level increases, age of menarche remains relatively stable (shown by a more horizontal red line)

Bubble plot of associations between plasma fluoride and age of menarche according to race/ethnicity. Size of bubbles reflects the magnitude of sampling weights. N = 504. Descriptive caption. The graph depicts 4 regression lines in different colors representing associations of plasma fluoride concentrations with age of menarche among 4 different racial/ethnic categories: Non-Hispanic White, Hispanic, Non-Hispanic Black and Other race/Multiracial. Plasma fluoride concentrations are depicted along the horizontal axis, while age of menarche is shown along the vertical axis. As plasma fluoride concentration increases, age of menarche decreases notably for Non-Hispanic Black participants (shown by a descending purple line), but remains relatively stable for the other racial/ethnic participant groups (shown by relatively straight horizontal lines)
Discussion
Fluoride exposure has been shown to disrupt endocrine function (NRC 2006); however, potential pubertal and reproductive impacts of fluoride exposure at levels relevant to the US population are poorly understood. This study explored associations of fluoride exposure with pubertal and reproductive health parameters among adolescent girls and women aged 16–19 in the US. We also examined whether race/ethnicity may modify associations of fluoride exposure with these parameters given that there are racial and ethnic differences in pubertal onset and reproductive health outcomes among US girls and women (Chumlea et al. 2003).
We did not observe any significant associations between fluoride exposure and menstrual cycle regularity or serum sex-steroid hormone levels. Our findings are consistent with a recent study using NHANES data that did not find significant associations of fluoride exposure with serum sex steroid hormone levels among adolescent girls and women ages 12–19 (Bai et al. 2020a, b). However, we found that higher water fluoride concentrations were associated with earlier age of menarche, such that each 0.53 mg/L increase in household tap water fluoride concentration was associated with approximately a 3.3-month-earlier age of menarche. This finding is somewhat consistent with a study by Schlesinger et al. (1956) which reported that the average age of menarche in Newburgh, New York, a city fluoridated for 10 years at 1.2 mg/L was 12 years, compared to 12.5 years in Kingston, NY, a non-fluoridated city, although these differences were not statistically significant. Conversely, we did not observe significant associations between plasma fluoride concentration and age of menarche among the overall sample in our study. This is consistent with a recent study conducted in Mexico City that did not observe significant associations between urinary fluoride concentrations and age of menarche or pubertal staging among 10–17-year-old girls (Liu et al. 2019a, b).
However, when we examined effect modification of the associations between plasma fluoride and age of menarche by race/ethnicity we found that higher plasma fluoride concentrations were associated with earlier menarche among Non-Hispanic Black adolescents only. Specifically, among Non-Hispanic Black adolescents, each 0.3 µmol/L increase in plasma fluoride was associated with a 5-month earlier age of menarche. Interestingly, a prior study utilizing NHANES data found that the median age of menarche for Non-Hispanic Black girls was earlier than for other racial/ethnic groups. Specifically, menarche occurred at 12.06 years for Non-Hispanic Black girls, 12.25 years for Mexican American girls and 12.55 years for Non- Hispanic White girls (Chumlea et al. 2003). A study conducted in Louisiana also found that the average age of menarche was 12.3 years among Black girls compared to 12.6 years among White girls. Additionally, they found that over a 20-year period, median age of menarche decreased by approximately 9.5 months among Black girls compared to approximately 2 months among White girls (Freedman et al. 2002). While research suggests that social factors such as racism (Prather et al. 2018), childhood stress (Mishra et al. 2009), lower household income (Braithwaite et al. 2009), and lower birth weight (Reagan et al. 2012) may partially account for these differences, variation in exposure to EDCs has also been proposed as a potential contributing factor to racial/ethnic disparities in women’s reproductive health outcomes (James-Todd et al. 2016). Notably, we observed higher water and plasma fluoride concentrations among Non-Hispanic Black adolescents compared to all other race/ethnicities in our NHANES sample, which could potentially explain some of the variance in our findings; however, future prospective studies are needed to explore potential health disparities in associations of fluoride exposure with age of menarche.
There are several mechanisms by which fluoride exposure could potentially impact female reproductive health. One potential mechanism is that fluoride has been shown to alter adrenal gland function in animals and this could impact hormone production and regulation (Shashi 2003). Additionally, fluoride can accumulate in the pineal gland and contribute to calcification (Kalisinska et al. 2014; Tharnpanich et al. 2016) which has been associated with decreased melatonin production (Kunz et al. 1999). Melatonin levels tend to fluctuate according to reproductive stage and decrease prior to the onset of puberty, suggesting that they may play an inhibitory role in pubertal onset (Macchi and Bruce 2004). Interestingly, a doctoral dissertation (Luke 1997) found that prepubescent gerbils fed a high fluoride diet had significantly lower melatonin production than those fed a low-fluoride diet and that female gerbils on the high fluoride diet reached sexual maturation more quickly. These and other potential mechanisms should be investigated in toxicological studies.
This study has several strengths including its large sample size representative of the US national population and use of individual biomarker measures of exposure. However, it also has limitations. First, it is cross-sectional, and assessment of age of menarche was recalled retrospectively which could be subject to recall biases as it relies on participant memory. However, given that our study included individuals who reported their age of menarche during adolescence, and therefore in relatively close temporal proximity between time since event and time of reporting, recall bias may be less influential. Additionally, research shows that women tend to recall age of menarche accurately, even 30 years later (Must et al. 2002). Furthermore, we expect any recall bias or forgetting to be nondifferential with respect to fluoride exposure. Second, ‘menstrual cycle regularity’ was defined as menstrual period having occurred once in the past 12 months and therefore did not reflect long-term patterns in menstrual cycle regularity or variability. Additionally, most participants in this study (i.e., > 95%) reported having a menstrual period during the past 12 months and thus there was little variability in this outcome which may limit detection of significant associations. Third, blood sample collection time was not standardized, and plasma fluoride concentrations can fluctuate due to daily behaviors that were not controlled for in this study (e.g., tea consumption; consumption of foods sprayed with fluoride-containing pesticides). This exposure misclassification could potentially bias associations toward the null. Fourth, NHANES did not measure stress-related variables and thus, we cannot rule out residual confounding or assess potential effect modification by stress or other psychosocial factors (Mishra et al. 2009; Prather et al. 2018).
Conclusion
Whether chronic low-level fluoride exposure may influence reproductive health outcomes in adolescents is an important area of study. Findings from this study, as well as health differences in potential reproductive impacts of fluoride, should be explored in prospective studies.
Data Availability
Data from NHANES is available online at https://wwwn.cdc.gov/nchs/nhanes/Default.aspx. The datasets generated during and/or analysed during the current study are available on reasonable request.
Code Availability
Code utilized for data analysis in this manuscript can be made available upon reasonable request.
References
Bai R, Huang Y, Wang F, Guo J (2020a) Associations of fluoride exposure with sex steroid hormones among U.S. children and adolescents, NHANES 2013–2016. Environ Pollut 260:114003
Bai R, Huang Y, Wang F, Guo J (2020b) Associations of fluoride exposure with sex steroid hormones among US children and adolescents, NHANES 2013–2016. Environ Pollut 260:114003
Bhasin S, Brito JP, Cunningham GR, Hayes FJ, Hodis HN, Matsumoto AM, Snyder PJ, Swerdloff RS, Wu FC, Yialamas MA (2018) Testosterone therapy in men with hypogonadism: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab 103(5):1715–1744
Braithwaite D, Moore DH, Lustig RH, Epel ES, Ong KK, Rehkopf DH, Wang MC, Miller SM, Hiatt RA (2009) Socioeconomic status in relation to early menarche among black and white girls. Cancer Causes Control 20(5):713–720
CDC (2017) Data sources and data analysis: blood, serum, and urine samples from NHANES. 2021. https://www.cdc.gov/exposurereport/data_sources_analysis.html. Accessed Oct 12 2021
CDC (2018a) Community water fluoridation. 2018 Fluoridation statistics. https://www.cdc.gov/fluoridation/statistics/2018stats.htm. Accessed April 5 2021
CDC (2018b) Laboratory procedure manual, total estradiol and total testosterone, NHANES 2015–2016
CDC (2018c) Laboratory procedure manual, sex hormone-binding globulin, NHANES 2015–2016
Centers for Disease Control and Prevention (2013) Specifying weighting parameters. https://www.cdc.gov/nchs/tutorials/NHANES/SurveyDesign/Weighting/intro_i.htm. Accessed 20 Nov 2018
Chaithra B, Sarjan HN, Shivabasavaiah, (2020) Sodium fluoride and fluoride contaminated ground water induced altered reproductive performances in male rats. Biol Trace Elem Res 195(2):544–550
Chen Q, Wang Z, Xiong Y, Liu D, Chen G (2015) The research on the relationship between the ovarian function damage with fluorosis and the protective effect of selenium. Value Health 18(7):A638
Chumlea WC, Schubert CM, Roche AF, Kulin HE, Lee PA, Himes JH, Sun SS (2003) Age at menarche and racial comparisons in US girls. Pediatrics 111(1):110–113
Duan L, Zhu J, Wang K, Zhou G, Yang Y, Cui L, Huang H, Cheng X, Ba Y (2016) Does fluoride affect serum testosterone and androgen binding protein with age-specificity? A population-based cross-sectional study in Chinese male farmers. Biol Trace Elem Res 174(2):294–299
Farkas G, Fazekas A, Szekeres E (1983) The fluoride content of drinking water and menarcheal age. Acta Univ Szeged Acta Biol 29(1–4):159–168
Freedman DS, Khan LK, Serdula MK, Dietz WH, Srinivasan SR, Berenson GS (2002) Relation of age at menarche to race, time period, and anthropometric dimensions: the Bogalusa Heart Study. Pediatrics 110(4):e43–e43
Greenspan LC, Lee MM (2018) Endocrine disrupters and pubertal timing. Curr Opin Endocrinol Diabetes Obes 25(1):49–54
Jain RB (2017) Concentrations of fluoride in water and plasma for US children and adolescents: data from NHANES 2013–2014. Environ Toxicol Pharmacol 50:20–31
James-Todd TM, Chiu Y-H, Zota AR (2016) Racial/ethnic disparities in environmental endocrine disrupting chemicals and women’s reproductive health outcomes: epidemiological examples across the life course. Curr Epidemiol Rep 3(2):161–180
Kalisinska E, Bosiacka-Baranowska I, Lanocha N, Kosik-Bogacka D, Krolaczyk K, Wilk A, Kavetska K, Budis H, Gutowska I, Chlubek D (2014) Fluoride concentrations in the pineal gland, brain and bone of goosander (Mergus merganser) and its prey in Odra River estuary in Poland. Environ Geochem Health 36(6):1063–1077
Kaplowitz PB (2008) Link between body fat and the timing of puberty. Pediatrics 121(Supplement 3):S208
Kinawy AA, Al-Eidan AA (2018) Impact of prenatal and postnatal treatment of sodium fluoride and aluminum chloride on some hormonal and sensorimotor aspects in rats. Biol Trace Elem Res 186(2):441–448
Kunz D, Schmitz S, Mahlberg R, Mohr A, Stöter C, Wolf K-J, Herrmann WM (1999) A new concept for melatonin deficit: on pineal calcification and melatonin excretion. Neuropsychopharmacology 21(6):765–772
Lee JE, Jung HW, Lee YJ, Lee YA (2019) Early-life exposure to endocrine-disrupting chemicals and pubertal development in girls. Ann Pediatr Endocrinol Metab 24(2):78–91
Li M, Cao J, Zhao Y, Wu P, Li X, Khodaei F, Han Y, Wang J (2020) Fluoride impairs ovary development by affecting oogenesis and inducing oxidative stress and apoptosis in female zebrafish (Danio rerio). Chemosphere 256:127105
Liu H (1988) Analysis of the effect of fluoride on male infertility in regions with reported high level of fluoride (endemic fluorosis). J Med Inst Suzhou 8(4):297–299
Liu L, Wang M, Li Y, Liu H, Hou C, Zeng Q, Li P, Zhao Q, Dong L, Yu X, Liu L, Zhang S, Wang A (2019a) Low-to-moderate fluoride exposure in relation to overweight and obesity among school-age children in China. Ecotoxicol Environ Saf 183:109558
Liu Y, Téllez-Rojo M, Hu H, Sánchez BN, Martinez-Mier EA, Basu N, Mercado-García A, Solano-González M, Peterson KE (2019b) Fluoride exposure and pubertal development in children living in Mexico City. Environ Health Global Access Sci Source 18(1):26–26
Lucaccioni L, Trevisani V, Marrozzini L, Bertoncelli N, Predieri B, Lugli L, Berardi A, Iughetti L (2020) Endocrine-disrupting chemicals and their effects during female puberty: a review of current evidence. Int J Mol Sci 21(6):2078
Luke JA (1997) The effect of fluoride on the physiology of the pineal gland. University of Surrey, Guildford
Macchi MM, Bruce JN (2004) Human pineal physiology and functional significance of melatonin. Front Neuroendocrinol 25(3–4):177–195
Malin AJ, Lesseur C, Busgang SA, Curtin P, Wright RO, Sanders AP (2019) Fluoride exposure and kidney and liver function among adolescents in the United States: NHANES, 2013–2016. Environ Int 132:105012
Martinez-Mier EA, Soto-Rojas AE (2010) Differences in exposure and biological markers of fluoride among White and African American children. J Public Health Dent 70(3):234–240
Mishra GD, Cooper R, Tom SE, Kuh D (2009) Early life circumstances and their impact on menarche and menopause. Women’s Health 5(2):175–190
Must A, Phillips S, Naumova E, Blum M, Harris S, Dawson-Hughes B, Rand W (2002) Recall of early menstrual history and menarcheal body size: after 30 years, how well do women remember? Am J Epidemiol 155(7):672–679
National Center for Health Statistics (2013) Overview of NHANES survey design and weights. https://www.cdc.gov/Nchs/tutorials/environmental/orientation/sample_design/index.htm. Accessed 21 Nov 2018
National Research Council (2006) Fluoride in drinking water: a scientific review of EPAs standards. The National Academies Press, Washington, DC
NHANES (2016a) 2013–2014 data documentation, codebook, and frequencies fluoride—water (FLDEW_H). https://wwwn.cdc.gov/Nchs/Nhanes/2013-2014/FLDEW_H.htm. Accessed 27 Dec 2019
NHANES (2016b) 2013–2014 data documentation, codebook, and frequencies fluoride—plasma (FLDEP_H). https://wwwn.cdc.gov/Nchs/Nhanes/2013-2014/FLDEP_H.htm. Accessed 27 Dec 2019
NHANES (2017a) 2015–2016 data documentation, codebook, and frequencies fluoride—water (FLDEW_I). https://wwwn.cdc.gov/Nchs/Nhanes/2015-2016/FLDEW_I.htm#Codebook
NHANES (2017b) National Health and Nutrition Examination Survey. 2015–2016 data documentation, codebook, and frequencies: fluoride—plasma (FLDEP_I). https://wwwn.cdc.gov/Nchs/Nhanes/2015-2016/FLDEP_I.htm. Accessed 27 Dec 2019
NHANES (2018) "National Health and Nutrition Examination Survey 2015–2016 data documentation, codebook, and frequencies sex steroid hormone—serum (TST_I)." https://wwwn.cdc.gov/Nchs/Nhanes/2015-2016/TST_I.htm. Accessed 27 Dec 2019
Orta Yilmaz B, Korkut A, Erkan M (2018) Sodium fluoride disrupts testosterone biosynthesis by affecting the steroidogenic pathway in TM3 Leydig cells. Chemosphere 212:447–455
Prather C, Fuller TR, Jeffries WL IV, Marshall KJ, Howell AV, Belyue-Umole A, King W (2018) Racism, African American women, and their sexual and reproductive health: a review of historical and contemporary evidence and implications for health equity. Health Equity 2(1):249–259
Reagan PB, Salsberry PJ, Fang MZ, Gardner WP, Pajer K (2012) African-American/white differences in the age of menarche: accounting for the difference. Soc Sci Med 75(7):1263–1270
Schlesinger E, Overton D, Chase H, Cantwell K (1956) Newburgh-Kingston caries-fluorine study. XIII. Pediatric findings after ten years. J Am Dent Assoc 52(3):296–306
Shashi A (2003) Fluoride and adrenal gland function in rabbits. Fluoride 36(4):241–251
Sifakis S, Androutsopoulos VP, Tsatsakis AM, Spandidos DA (2017) Human exposure to endocrine disrupting chemicals: effects on the male and female reproductive systems. Environ Toxicol Pharmacol 51:56–70
Susheela AK, Jethanandani P (1996) Circulating testosterone levels in skeletal fluorosis patients. J Toxicol Clin Toxicol 34(2):183–189
Tharnpanich T, Johns J, Subongkot S, Johns NP, Kitkhuandee A, Toomsan Y, Luengpailin S (2016) Association between high pineal fluoride content and pineal calcification in a low fluoride area. Fluoride 49(2):472–484
U.S. Department of Health & Human Services. (2013-2016) U.S. Department of Health & Human Services Poverty Guidelines, Research and Measurement. Department of Health & Human Services, Washington DC
United States Department of Health and Human Services -Federal Panel on Community Water Fluoridation (2015) US Public Health Service recommendation for fluoride concentration in drinking water for the prevention of dental caries. Public Health Rep 130(4):318–331
US Environmental Protection Agency (USEPA) (2010) Fluoride: exposure and relative source contribution analysis. US Environmental Protection Agency, Health and Ecological Criteria Division, Washington, DC
Villa A, Anabalon M, Zohouri V, Maguire A, Franco A, Rugg-Gunn A (2010) Relationships between fluoride intake, urinary fluoride excretion and fluoride retention in children and adults: an analysis of available data. Caries Res 44(1):60–68
Acknowledgements
We gratefully acknowledge Heather Burris, MD, MPH for her careful review of our manuscript and helpful feedback. We would also like to thank participants and staff of the NHANES without whom this research would not have been possible.
Funding
This work was supported in part by funding from The National Institute of Environmental Health Sciences (NIH/NIEHS): R00ES027508; K99ES031676.
Author information
Authors and Affiliations
Contributions
AJM: Conceptualization; Data curation; Formal analysis; Funding acquisition; Investigation; Methodology; Project administration; Software; Supervision; Validation; Visualization; Writing—original draft; Writing—review & editing; SAB: Data curation; Formal analysis; Investigation; Methodology; Software; Validation; Visualization; Writing—review & editing; JCG: Investigation; Writing—review & editing; SB: Conceptualization; Writing—review & editing; APS: Conceptualization; Funding acquisition; Investigation; Methodology; Project administration; Supervision; Visualization; Writing—original draft; Writing—review & editing.
Corresponding author
Ethics declarations
Conflict of interest
The authors of this manuscript do not have any conflicts of interest to disclose.
Ethical Approval
This study was exempt from review by the Icahn School of Medicine at Mount Sinai’s (ISMMS) Institutional Review Board (#1702145).
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Malin, A.J., Busgang, S.A., Garcia, J.C. et al. Fluoride Exposure and Age of Menarche: Potential Differences Among Adolescent Girls and Women in the United States. Expo Health 14, 733–742 (2022). https://doi.org/10.1007/s12403-021-00448-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12403-021-00448-y